Comlr Ssion Socks and Knee Sleeve at Aame Time
Socket Casting, Positive Mould, and Rectification [edit | edit source]
The prosthetic socket is the primary and critical interface between the amputee's residual limb and the rest of the prosthesis,[1] [2] and therefore a good, comfortable fit is required to ensure a positive outcome is reached in an amputees rehabilitation[2]. The socket has to be efficiently fitted, have adequate load transmission, and it needs to ensure stability and control[1]. Many patients with amputations stop wearing their prosthesis and a major cause is socket-related problems (poor fit, poor biomechanics, and reduced control)[1].
The process of making a socket begins with taking measurements and a negative cast of the residual limb. The cast is filled with plaster to create a positive mould. The positive mould is then modified to optimize the socket fit, this process is called "rectification". The socket is then laminated using carbon and resin to create the custom socket, this is referred to as the definitive socket. A "check"/test/diagnostic socket is sometimes fabricated before creating the definitive socket (this socket is usually transparent, allowing the clinician a complete view to evaluate the fit and make changes). Multiple fittings are at times necessary to assure the best possible design with a comfortable and effective fit. Generally, test sockets are made out of plastic. Definitive sockets are laminated and can be made with fibreglass, carbon fibre, or nylon materials[3].
Because it is the interface between the device and residual limb, the quality of the socket design, whatever the model used, is key and decides on user's comfort and his/her ability to control the appliance. A user will never walk properly and will never reach the agreed goal of the rehabilitation plan if the quality of the socket fit is not satisfactory regardless of the material used (plastic, resin or carbon). The quality of the fit depends entirely on the work of the prosthetist and his/her capacity to ensure precise measurements during casting and suitable rectification of the positive mould to distribute forces over the socket where needed.
Other methods: [edit | edit source]
- Polypropylene technology developed by the International Committee of the Red Cross (ICRC) is used in prosthetics all over the world, especially in resource-limited countries and projects by the ICRC. Polypropylene is used in the US also as an alternative to laminating a definitive socket. It is cheaper than laminating but can be just as durable.
- The Modular Socket System developed by Ossur can be used to make a socket directly on the patient's residual limb. It is an easier and quicker process but the cost is higher. Delivery time to the patient could be within one day. [6] This is currently available for transtibial amputees.
- A more sophisticated and expensive technique utilized today is a CAD system (Computer Aided Design). With the improvement of technology 3D printed sockets are also gaining momentum.
- Adjustable sockets are gaining more popularity, such as the RevoFit2 Adjustable Socket.
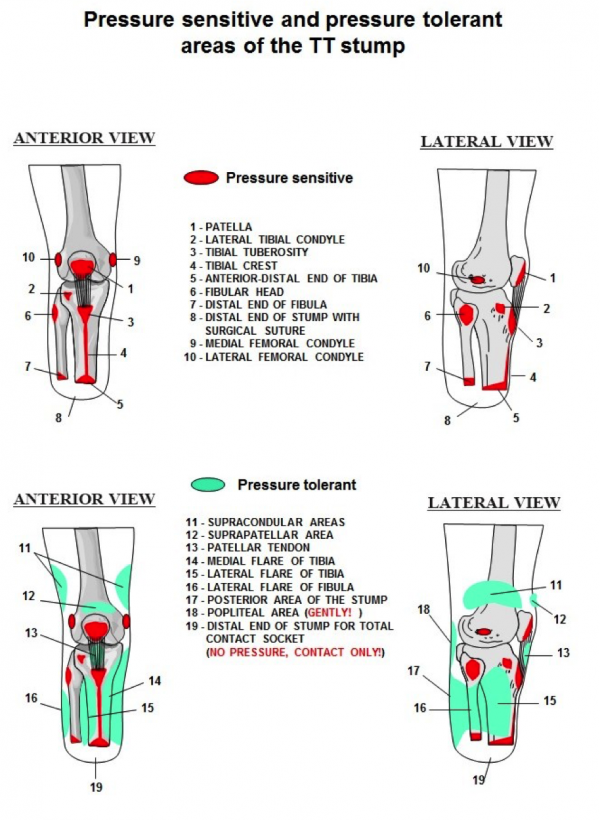
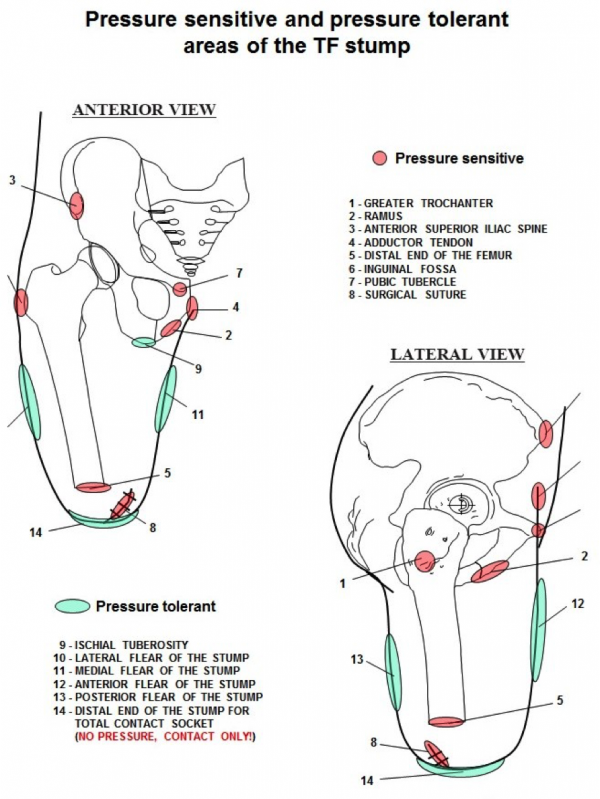
Pressure tolerant and pressure-sensitive areas: [edit | edit source]
The socket applies external forces over the surface of the residual limb. The amount, the location of their application and the means that control those forces contributes to the impact the prosthesis has on mobility, function, and acceptance of the device. Pressure distribution over a greater surface diminishes the load and provides more comfort during the use of prosthesis.
Although the majority of the stump areas are considered as pressure tolerant, some are very sensitive and cannot support any pressure. Sockets designs should allow forces to be distributed over as large a residuum surface area as possible and should be applied as evenly as possible over pressure-tolerant areas. These pressure-tolerant areas might turn red with pressure, that will subside when the prosthesis is taken off, but no skin breakdown occurs. Pressure-sensitive areas have a high probability of skin breakdown. No redness should occur in the pressure-sensitive areas. Knowing these areas will help the therapist to know where some redness is normal in a properly fitted socket. When redness occurs at pressure-sensitive areas the therapist should consult with the prosthetist.
You can listen to this podcast to learn more.
Attention:
Very short TT stumps (shorter than 20% of the anatomical length) are insufficient for providing adequate control over the prosthesis and supporting the body weight. Nevertheless, the quality of the stump is more important than its length.
The purpose of the socket is to provide structural integrity to the prosthesis where it interfaces with the residual limb. It also may provide elements of suspension to hold the prosthesis in place. The socket should be comfortable and able to withstand all of the external forces placed upon it by the user.
Below we describe some common TT and TF socket designs.
Transtibial Sockets [edit | edit source]
Patellar Tendon Bearing [edit | edit source]
| Socket PTB (Patellar Tendon Bearing) The weight bearing takes place below the patella, at the patellar tendon. The suspension is generated by a belt that is tightened around the distal part of the thigh. The tension of that belt limits the blood and lymphatic circulation; moreover, after long term use results in muscle atrophy and other related problems. | |
| Socket PTB SC (Patellar Tendon Bearing Supracondylar) The weight bearing takes place below the patella, at the patellar tendon. The suspension is generated at the medial and lateral areas of the femoral condyles. Compared to the PTB socket with belt suspension, this design does not produce problems of blood circulation or atrophy. For the moment, this type is used worldwide as most basic design for prosthetic fitting of medium and long stumps. | |
| Socket PTB SC SP (Patellar Tendon Bearing Supracondylar Suprapatellar) The weight bearing takes place below the patella, at the patellar tendon. The suspension is generated at the medial and lateral areas of the femoral condyles and at the suprapatelar area. This type is indicated for short stumps, as well as in cases of antero-posterior instability in the knee. | |
Indications
Primary Amputees - The PTB socket is good for primary amputees as the socket can be modified to accommodate the changes in the residual limb that occur for 12-18 months after the amputation.
- Sensitive Residual Limbs - If the amputee has a particular area of sensitivity on their residuum it is possible in a PTB socket to relieve these areas more easily than in a total surface bearing style socket.
- Bulbous Residual Limbs - The construction of a PTB socket, an inner liner and outer hard socket, allows for build-ups to be applied to the inner liner allowing easier donning and doffing for an amputee with a bulbous residual limb
- Poor Hand Dexterity/ Poor Eyesight/ Hemiparesis - PTB sockets are much easier to don/doff than total surface bearing sockets
Contraindications
- Active amputees can find the PTB trim lines and suspension methods too restrictive, especially with regards to knee flexion.
- Some amputees can find the PTB prosthesis pistons (see pistoning in gait deviations)
- Some amputees cannot tolerate the pressure on their patella tendon required for a PTB prosthesis to work effectively.
Total surface bearing sockets [edit | edit source]
| Socket SSS (Silicon Suction Socket) The weight bearing takes place all over the stump surface. The suspension is generated by means of tight adhesion/friction between stump and silicon liner that has a pin at its distal part. This pin is installed in a blocking mechanism inside the prosthetic components, or using a suction mechanism, hence insuring the suspension. Indicated for all types of stumps. | |
- TSB sockets "uniformly distribute weight over the entire residual limb" which therefore "delivers a minimal skin pressure"[10].
- TSB sockets are volume matched to the residual limb with 100% surface contact during the gait cycle.
- Successful fitting of a TSB socket requires good control of the soft tissues, minimised pressure peaks and distribution of load over the maximum surface area available[11].
Advantages and Indications
- Active amputees benefit from the lower trim lines possible with the TSB style design[10] [12] .
- TSB sockets reduce pistoning of the socket (see pistoning in gait deviations) on the residual limb by providing total contact throughout the gait cycle[13]
- Proprioception is increased due to weight bearing over the entire residual limb and good pressure distribution by the socket walls, which in turn enables the amputee to have better balance with eyes open or closed[13]
- Suspension of the TSB socket is also noted to be better than the PTB design as it is integrated in the socket using locking pins or suction[13].
- Due to the entire surface of the residual limb accepting weight in the TSB socket it is believed that these sockets are more comfortable because overall socket pressure is reduced[14].
Disadvantages and Contraindications
- TSB sockets are not suitable for primary amputees due to volume changes in the first 12-18 months post-amputation[15]. For the same reason TSB sockets are also not suitable for amputees undergoing treatments such as dialysis due to volume fluctuation
- Unsuitable for patients with short residual limbs, less then 10cm long, which require higher trim lines for stability around the knee[12].
- Some amputees may experience pain at the distal end of their residual limb due to the way a TSB/HST socket weight bears over the entire limb[15]. Also patients with excessive soft tissue may drop down into a TSB/HST socket too much which will cause pain at the distal end[15]. Amputees with bony spurs are also not suitable for TSB/HST sockets[15].
- Discomfort during knee flexion may result due to the silicon liner bunching up in the popliteal region[16]
- Increased perspiration may result due to the silicon liner, which can lead to irritation of the residual limb[16]
- TSB/HST sockets are not indicated for amputees with visual/sensory disturbances or Hemiparesis as they are more difficult to don/doff than a PTB design[15].
- Amputees with excessive soft tissue may find they get discomfort upon knee flexion due to creasing of the silicon liner[15]
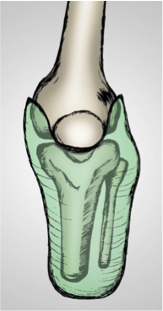
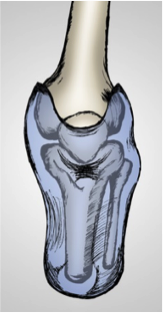
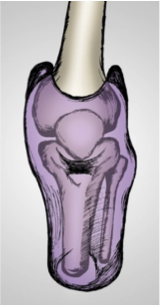
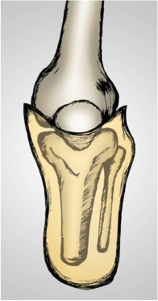
Transversal view shows the differences between the internal shapes of PTB SC v SSS sockets.
| Socket PTB SC | Socket SSS |
| | |


Transfemoral Sockets [edit | edit source]
For TF sockets, the designs mostly used at present are the followings.
Quadrilateral Socket [edit | edit source]
The weight bearing takes place at the ischial tuberosity by the means of ischial support at the posterior shelf of the socket. The suspension is provided by negative pressure (suction) that is generated by adequate fitting of the socket over the stump. In some cases, the suction suspension can be complemented by the use of the belts (Silesian, Neopren, etc.).
For the moment, this type of socket is in most use for all types of stumps.
| Transversal view | Medial view | Posterior view |
| | ||

Ischial Containment Socket [edit | edit source]
The weight bearing takes place all over the surface of the stump without localizing one specific point; hence, generating more comfort, better control over the prosthesis and security for the user. The ischial tuberosity does not suffer from direct, complete and permanent weight bearing. The principal peculiarity of this design, apart of the exact volume determination, is the medial wall/border of the socket that contains the ischial ramus. The suspension is provided by negative pressure (suction) generated by adequate fitting of the socket over the stump.
For the moment, this type of socket is in worldwide promotion, replacing the quadrilateral one.
Transversal view Medial view Posterior view
| Transversal view | Medial view | Posterior view |
| | ||

[17]
Suspension Systems [edit | edit source]
This is a crucial factor in the design of a prosthesis. The suspension is how the socket kept on the residual limb preventing it to fall off when the leg is lifted up or moved during gait. Good suspension will improve the energy transfer, enhance the control of the prosthesis, and decrease any discomfort or abrasions. When suspension is poor the leg will feel heavy and may lead to skin breakdown. For suspension prescription the patient will need to be thoroughly assessed not just with regard to the residuum shape and length, but also their overall strength, hand dexterity, eye sight, and balance in standing. [3]
[18]
1.Cuffs, Straps and Belts [19] [edit | edit source]
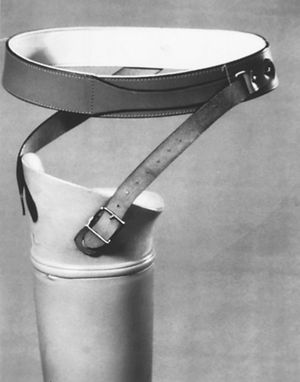
Also called Auxillary suspension. This is the original way of keeping the socket on and prevent it from falling off during the swing phase. Even though this and "old" way of suspension it is still used today as it is an inexpensive, simple, reliable and durable way of suspension. This can vary from a simple soft strap/cuff to a very rigid band around the pelvis.
- Transtibial: With PTB sockets there can be a strap over the patella.
- Transfemoral: Belts or straps can be used as a primary suspension method if other methods fail or are not appropriate. It can also be used as a secondary option for when negative pressure or suction is used. It is also indicated for an individual with a short residuum, who have changing volume of their residuum, this keeps the socket on even if the socket fit is loser at the end of the day or poor hip abductor strength. Disadvantages: It is warm, pressure around the pelvis area, needs good hand dexterity and strength, moves when sitting, uncomfortable, provides minimal suspension, can cause bruising or chafing.
2. Lanyard[19] [edit | edit source]
This is when a cord or strapped is attached to lower end of the liner. As the individual inserts the residuum with the liner on the cord/strap will go through a small hole in the bottom of the socket. The cord is then pulled tight, to draw the residuum into the socket. The lanyard is then attached with a mechanism on the outside of the prosthesis to keep it secure. Used for transfemoral suspension.
- Advantage: Easy to don (put on) the prosthesis in a seated position, especially for someone with poor eyesight or balance. It provides a secure suspension and decreases socket rotation. Inexpensive, simple, and reliable.
- Disadvantages: Needs some hand dexterity and strength. A liner is needed for suspension.
3. Self Suspending Socket[19] [edit | edit source]
This is when the suspension is created by the socket brim (top part) on the residuum. The brim part is made to extend and narrow over the joint (example over the knee joint) in order to create a grasp or hold over the joint. An example of this is the Patellar Tendon Bearing Supracondylar Socket. Only for transtibial suspension. Poor Suspension. For more information read the part Patellar Tendon Bearing Sockets higher up on this page.
4. External Sleeve[19] [edit | edit source]
A sleeve that fits snugly over the socket and then extends onto the individual's thigh is used to seal in the air in the socket and in that way create a suspension. Sleeves are made from different materials including neoprene, silicone or copolymer gel. Mostly used with transtibial sockets.
- Advantage: Pistoning (movement of the residuum inside the socket) is reduced with an airtight seal. Sleeves are flexible and usually allows the knee to bend (if the sleeve has a ribbed or wave design over the knee joint) and it is cosmetic as it covers the top edge of the socket. It is a reliable form of suspension and relatively inexpensive.
- Disadvantages: Sleeves without a ribbed or wave design can cause abrasion over the patella. If applied incorrectly the person can get a skin irritation where the sleeve touches the skin. Needs hand dexterity and strength. The sleeve's effectiveness is reduced with wear and tear, a hole in the sleeve can lead to a loss of suction.
[20]
5. Pin and Lock[19] [edit | edit source]
A silicon or gel liner with a pin at the bottom of the liner is used on the residual limb. When the limb is placed into the socket the pin has to go into a locking mechanism at the bottom of the socket. This mechanism will lock the pin in place, creating a secure suspension in the socket. It is used in both transfemoral and transtibial prosthetics. A release mechanism can be pressed to unlock the pin.
- Advantages: Provide a positive mechanical lock with auditory feedback for the user when the pin engages. Relatively easy donning and doffing and can be done in a sitting position. More forgiving with volume fluctuations.
- Disadvantages: Due to the pulling down action of the pin on the liner an elongation effect can happen at the bottom of the residuum and cause skin breakdown, but newer liners are reinforced with a matrix to avoid this from happening. Wear and tear on liners. When the pin is misaligned or the liner is donned incorrectly the locking mechanism will not be engaged, this might be difficult for someone not having the ability to bend down or with poor eyesight.
[21]
6. Suction without a liner[19] [edit | edit source]
The socket is made with an expulsion valve that will let the air out to create a seal once the residuum is in and the valve is closed. The suction is created between the bare skin and the inside of the socket. To achieve this, the individual will have to pull the residuum into the socket using a piece of material, a special sock, cord or webbing. By opening or pushing on the suction valve the air will return, breaking the seal and thereby releasing the residuum to remove the prosthesis.
- Advantage: With an accurate fit the suspension will be very good. Less expensive than options with liners
- Disadvantage: When the socket is donned poorly the suction will not hold and there will be poor suspension. It is an old way of suspension. Donning can be complex for some individuals as it requires hand strength and dexterity as well as balance in standing. Not secure suspension with volume fluctuations or if there is a failure with the valve.
7. Suction with a liner [3] [19] [edit | edit source]
A liner that is donned on the residuum is used to create suction instead of the skin suction described above. These liners are usually made of silicone or gel, to create a seal with the inside of the socket the liner can have silicone rings/ribs or a membrane. The air can escape through the valve as the socket is donned and will keep the suction once the valve is closed. Some sockets have a one-way valve. By opening or pushing on the suction valve the air will return, breaking the seal and thereby releasing the residuum to remove the prosthesis. Lubricant or an alcohol solution on the seal will help the liner to slide in and to create a seal. When using suction with a liner an external sleeve is not necessary, unless there are severe volume fluctuations. The liner is usually covered with material to help it last longer.
- Advantage: Even pressure throughout the socket. Secure fit. Donning in a seated position is possible. Used to stabilize excess residual tissue. Good suspension even with small volume fluctuations. Liner and socket donning does not have to be as precise to secure suspension but may cause rotation in the socket.
- Disadvantage: Relatively expansive. Wear and tear on liners. Poor suspension with significant volume fluctuations. Good hand strength and dexterity needed. Lubricant is needed for donning.
8. Vacuum-Assisted Suspension[19] [edit | edit source]
Also known as Negative Pressure, Elevated Vacuum or Dynamic Vacuum. Suction suspension is created with direct contact between the liner (or with the membranes on the liner) and the socket wall. With this system a mechanism/pump sucks the air out between the liner and the socket creating a negative pressure that is the same across the entire surface. To seal off the system an external sleeve or seal is used at the top of the socket.
- Advantage: The mechanism creates a constant negative pressure and allows for better suspension when there is volume fluctuation. Less pistoning and rotation occur within the socket.
- Disadvantage: More expensive. Mechanical components that can break. Adds weight to the prosthesis.
9. Osseointegration[19] [22] [edit | edit source]
This procedure can be done on patients with a short above knee amputation. An implant is placed within the remaining femur bone. When it is healed and the bone attached to the implant an osseointegrated prosthesis can be directly attached to the implant in the bone. No need for a socket or liner.
- Advantages: Physiological weight-bearing, better mobility because the socket is not restricting. Easy donning and doffing. Osseoperceptive sensory feedback that allows for more precise control over the prosthesis.
- Disadvantages: Cost of surgery and specific components for the prosthesis. Risk of infection and other complications such as delayed wound healing or bodily fluid leakage from the implant. Extensive rehabilitation is needed. With some implants, no weight bearing is allowed for 6 months.
This website is a great resource to see the different types of suspensions available as well as a list of manufacturers and the names of the components in each category.
More information on different types of liners.
[23]
Stump Socks [edit | edit source]
Stump socks can be added over the residuum or over the liner to provide additional circumference if the residuum change in volume. This will prevent movement within the socket, peak pressure points, and chafing. Socks can be made in different thicknesses from different materials like wool, cotton, nylon or socks impregnated with gel.
[24]
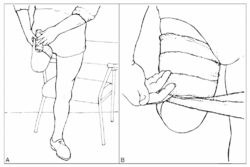
Donning and Doffing of Liners and Sockets [edit | edit source]
Donning a prosthesis refers to the application of a prosthetic device, doffing refers to the act of removing a prosthetic device.
There are many different types of prostheses available and the process of donning and doffing each is different. You will individually need to become familiar with the types of prosthesis that you use but these videos below provide some insight into donning and doffing socks, liners and prosthetics:
References [edit | edit source]
- ↑ 1.0 1.1 1.2 Paternò L, Ibrahimi M, Gruppioni E, Menciassi A, Ricotti L. Sockets for limb prostheses: a review of existing technologies and open challenges. IEEE Transactions on Biomedical Engineering. 2018 Jan 23;65(9):1996-2010.
- ↑ 2.0 2.1 Fergason J and Smith D.G (1999) Socket Considerations for the Patient With a Trans-Tibial Amputation Clinical Orthopaedics and Related Research 361 pages76-84
- ↑ 3.0 3.1 3.2 Engstrom B, Van de Ven C, editors. Therapy for amputees. Elsevier Health Sciences; 1999
- ↑ AmputeeOT: How a test prosthetic socket is made. Available from: https://youtu.be/zKib_5eDYUo [last accessed 01/01/18]
- ↑ Shriners Prosthetics BK socket lamination. Available from: https://youtu.be/DngKz0CYQLQ [last accessed 01/01/18]
- ↑ Normann E, Olsson A, Brodtkorb TH. Modular socket system versus traditionally laminated socket: a cost analysis. Prosthetics and orthotics international. 2011 Mar 1;35(1):76-80.
- ↑ ICRC PRP Cambodia Battambang's Prosthetic Workshop Transtibial Prosthesis . Available from: https://youtu.be/Oxez1AL34-8
- ↑ ICRC PRP Cambodia Battambang's Prosthetic Workshop - Transfemoral Prosthesis. Available from: https://youtu.be/ou4fqBrAm5g
- ↑ Modular Socket System by Össur. Available from: https://youtu.be/iLbGWjei4zY [[last accessed 06/02/20]
- ↑ 10.0 10.1 Kahle J.T (1999) Conventional and Hydrostatic Transtibial Interface Comparison Journal of Prosthetics and Orthotics 11(4) 85-91
- ↑ Muller M, Staats T.B, Leach M and Fothergill I , Total Surface Bearing Trans-Tibial Socket Design Impression Techniques
- ↑ 12.0 12.1 Söderberg B (2002) Technical Note: A New Trimline Concept for Trans-Tibial Amputation Prosthetic Sockets Prosthetics and Orthotics International 26 159-162
- ↑ 13.0 13.1 13.2 Yiğiter K, Şener G and Bayar K (2002) Comparison of the Effects of Patellar Tendon Bearing and Total Surface Bearing Sockets on Prosthetic Fitting and Rehabilitation Prosthetics and Orthotics International 26 206-212
- ↑ Moo E.K, Osman N.A.A, Pingguan-Murphy B, Wan Abas W.A.B, Spence W.D and Solomonidis S.E (2009) Interface Pressure Profile Analysis for Patella Tendon Bearing Socket and Hydrostatic Socket Acta of Bioengineering and Biomechanics 11(4) 37 – 43
- ↑ 15.0 15.1 15.2 15.3 15.4 15.5 Hachisuka K, Dozono K, Ogata H, Ohmine S, Shitama H, Shinkoda K (1998) Total Surface Bearing Below – Knee Prosthesis: Advantages, Disadvantages and Clinical Implications Archives of Physical Medicine and Rehabilitation 79 783-789
- ↑ 16.0 16.1 Sewell P, Noroozi S, Vinney J and Andrews S (2000) Developments in the Trans-Tibial Prosthetic Socket Fitting Process: A Review of Past and Present Research Prosthetics and Orthotics International 24 97-107
- ↑ Cornerstone Prosthetics and Orthotics. What Are Your Above Knee Amputee Options? Available from: https://youtu.be/nRzIWANwey0
- ↑ Bulow Orthotic and Prosthetic Solutions. Prosthesis Suspension Types Available from: https://youtu.be/uLlXvr4pzvI
- ↑ 19.0 19.1 19.2 19.3 19.4 19.5 19.6 19.7 19.8 NZALS Peke Waihanga, Aotearoa. Suspension Systems. https://www.nzals.co.nz/products/categories/suspension-systems
- ↑ Ottobock. How to put on a below knee prosthesis with one-way valve and knee sleeve?Available from:https://youtu.be/hwUF_DPXLPA
- ↑ Ottobock. How to put on an above knee prosthesis with Pin Liner (Shuttle Lock System)? Available from: https://youtu.be/nRC47UhXO0U
- ↑ Li Y, Brånemark R. Osseointegrated prostheses for rehabilitation following amputation. Der Unfallchirurg. 2017 Apr 1;120(4):285-92.
- ↑ AmputeeOT: Liner Primer! All about liners for prosthetic legs Available from: https://youtu.be/ySP7PXUloXE
- ↑ AmputeeOT: All about stump socks for below knee amputees. Available from: https://youtu.be/e22I_sG8q1A
- ↑ Saskatchewan Health Authority - Regina and Area. Donning and Doffing of Gel Liners. July 2014. Available from: https://youtu.be/-15YzvJduQI [last accessed 08/01/2020]
- ↑ Bulow Orthotic and Prosthetic Solutions. How to Don and Doff your Prosthesis. Available from: https://youtu.be/ncktp4NaZWk [last accessed 08/01/2020]
- ↑ alexschwarz76. Amputee putting on above knee prosthesis. March 2013. Available from: https://youtu.be/-5CobQYRNbY [last accessed 08/01/2020]
- ↑ AmputeeCoalition. AmputeeOT: How to take off and put on an Above Knee Prosthetic Leg. July 2014 Available from: https://youtu.be/pq890DFQh5Y [last accessed 08/01/2020]
- ↑ Renee Shadley. Revofit Adjustable Socket : Overview video for BKA amputee after amputatin. Jan 2017. Available from: https://youtu.be/_z0b-lkw8yw [last accessed 08/01/2020]
- ↑ SCProsthetics. Amputee dons Stan Patterson NPS Elevated Vacuum Above Knee Socket Tutorial. April 2010. Available from: https://youtu.be/r69ROFbPqaM [last accessed 08/01/2020]
Comlr Ssion Socks and Knee Sleeve at Aame Time
Source: https://www.physio-pedia.com/Lower_Limb_Prosthetic_Sockets_and_Suspension_Systems
Belum ada Komentar untuk "Comlr Ssion Socks and Knee Sleeve at Aame Time"
Posting Komentar